A project designed and implemented by the New Hampshire Pediatric Improvement Project and funded by the New Hampshire Children’s Health Foundation as part of its Childhood Adversity Systems Change Project//
Research has demonstrated that Adverse Childhood Experiences (ACEs) may have significant short and long-term effects on the health and well-being of children, adolescents and teens.
In 2012, the American Academy of Pediatrics released a policy statement outlining the critical role of the medical home in identifying and responding to ACEs. In 2018, the New Hampshire Pediatric Improvement Partnership released a report that identified challenges to implementing this recommendation in New Hampshire pediatric clinics, and recommendations for clinics to address them.
Recommendations included:
- Providing clinician training on trauma-informed care.
- Increasing public awareness about ACEs and Social Determinants of Health.
- Conducting research to help clinics operationalize team-based care to address ACEs.
What is a Trauma Informed Pediatric Practice?
The Childhood Adversity Screening in Primary Care project created and implemented by the New Hampshire Pediatric Improvement Partnership and funded by the New Hampshire Children’s Health Foundation was designed to advance these three recommendations.
“First, this project is increasing awareness and knowledge of NH pediatric and family practice clinicians and staff about childhood adversity – what it is, its health impact, and how to prevent or mitigate harmful impacts,” noted Holly Tutko, project director.
“Second, childhood adversity screening is relatively nascent and can be challenging,” she added. “This project is demonstrating how to support childhood adversity screening across a range of clinic types to identify and spread best practices.”
A Trauma Informed Pediatric Practice recognizes the impact of adverse childhood experiences on children and families, routinely screens for trauma exposure and related symptoms using evidence-based assessments, and collaborates with and refers families to child-serving systems in the local community.
While screening children for trauma and connecting them with resources to help them overcome it seems to make good sense, structural barriers stand in the way of wide-spread adoption by clinicians.
“Pediatric primary care has a high volume of patients as well as many requirements for most visits such as developmental screening, inoculations and so on. Fitting another requirement in can be tricky,” said Felicity Bernard, project director at the UNH Institute for Health Policy and Practice which operates the Pediatric Improvement Project.
“And, there’s no insurance reimbursement for it, which is a negative in terms of the financial viability of taking the time to invest in the training and systems needed to set it up,” Bernard added.
“This was the case with developmental screening. Some pediatricians were screening because it was a best practice, but a vast majority of folks waited until it was required and paid for before adopting it. Now it is universally done,” she said.

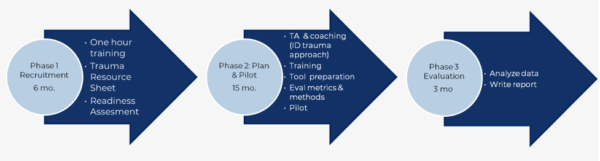
Introductory training
During the first phase, the project provided a free introductory training about adverse childhood experiences at 13 pediatric practices across Manchester, Nashua, the Monadnock Region, Concord and Coos County.
The one-hour, on-site presentation was delivered by a psychologist with a background in ACEs at participating clinics in the target communities. It provided an overview of ACEs, the impact of toxic stress on child development, and principals of trauma-informed care. The sessions were attended by 191 staff members and free continuing education credits were provided for attendees.
Facilitation and coaching
Five pediatric practices that participated in the Phase 1 introductory education requested to enroll in Phase 2 and were accepted based on meeting a criteria checklist. This next phase engaged them in 15 months of practice facilitation and coaching to support them in planning, piloting and adopting trauma-informed workflow changes.
Each clinic was assigned a skilled practice facilitator for the duration of the process. During the first nine months the facilitator walked the clinic team through a guide developed by project staff to answer four key questions:
- Who to screen.
- Selection of an evidence-based screening tool.
- How to implement the screening tool.
- What to do with results.
Dr. Brian Beals is a pediatrician at Coos County Family Health Services in Gorham one of the practices that volunteered to participate in Phase 2.
“We had long-recognized the negative impact of acute and chronic trauma on the health of the kids and families we work with every day,” said Dr. Beals. “We knew that systematic routine screening would help bring that to the forefront more efficiently and help us be proactive instead of reactive.
Dr. Beals noted that preventative strategies are the hallmark of pediatric well child care.
Concurrently, each clinic team completed a trauma-informed care site assessment to identify opportunities for the clinic to strengthen their use of trauma-informed care principles. The facilitator then supported the clinic in selecting strategies to address priorities that were identified.
During this time, project staff also coordinated meetings of the clinic team with local family support resources. These meetings served to enhance clinic knowledge about available resources in the community like the community mental health center, the family resource center, resources for survivors of domestic violence and the community action program.
Making connections with referral agencies not easy
Project staff discovered that clinic teams needed more assistance than anticipated with brokering connections with local referral sources and found that they needed to facilitate those discussions.
Felicity Bernard noted, “My feeling is that there are metaphorical ‘language and cultural’ issues at play here. Not in the traditional sense, but in ‘medical’ speak versus community support vocabulary. There also seemed to be operational and referral process differences that were not easily bridged. I did feel like a translator at times.”
Bernard also pointed to historic relationships between agencies and clinics. Unfortunately, one bad interaction years ago could be generalized to normal operations.
“I suspect high rates of turnover are the driving force behind this,” Bernard said. “What was happening at a community mental health center a year ago, may not be happening now.”
In addition, Bernard discovered that an enormous initial barrier here was finding the right person to talk to at a community agency. Then reaching that person and coordinating a time that worked for them and clinical staff to meet took much more effort than she anticipated.
The effort to connect primary care practices to community resources was worth it however.
“It’s the number one eye opening experience about this whole thing,” said one participating clinician. “We are learning about resources in the community that we’ve never known before. I have already started utilizing a lot of that. It’s not just about counseling.”
Plan-do-study-act
For the final six months of the project’s Phase 2, the project facilitator met monthly with each clinic team to support the use of quality improvement science, including plan-do-study-act cycles to their screening and response workflows and to review updated performance data.
During this time, clinics were also provided access to trauma and psychiatry experts for provider-to-provider patient consults.
Coos County Family Health Services has made a number of changes at its practice ranging from something as simple as hanging posters in all their exam rooms and restrooms asking basic trauma questions about whether anything “bad” or “scary” has happened, or if people feel safe, to make it clear that they are ready to help.
They have adopted routine screening for caregiver trauma when babies are 4 months old, then directly for child trauma at 3 years, 7 years and 13 years.
“Families can of course opt out,” said Dr. Beals, “but I have only had one family ever decline to answer some of the questions. In fact, many families go to the other extreme and thank us for asking how they are adjusting.
“Even when what is reported does not rise to the level of needed services it still serves as a nice starting point for what can otherwise be difficult conversations and as such help us provide more meaningful anticipatory guidance,” Dr. Beals said.
“For example if we learn that a parent had been exposed to domestic violence or other trauma in their own childhood we can use that knowledge to frame our discussion about tantrums which in those situations might trigger a parent should the toddler start hitting and make what is ‘normal’ behavior seem like something much bigger than it actually is,” he added.
Based on clinic need, three advanced trauma trainings were provided about provider resilience, trauma and its impact on families and a case study featuring a Maine primary care clinic’s organization of its ACE/trauma screening.
Phase 2 evaluation focused on assessing the impact of and clinic satisfaction with the fifteen-month process. Facilitators also worked with each clinic to determine how they would collect and submit data monthly for performance metrics. Phase 3 of the project entailed conducting quality assurance checks, data analysis and report writing.
“At the beginning some clinic teams were a bit overwhelmed, but with the coaching and tools they, found childhood adversity screening quite feasible,” said UNH’s Holly Tutko. “Clinics were often surprised about the array of family supports available locally. Most importantly, screening sparked new conversations to better understand how to help families thrive,” she said.
“Our agency has resources that others may not—a medical social worker, two counselors, crisis advocates and medical home personnel,” Dr. Beals said. “This project serves as a nice bridge to help make those connections earlier than we might have otherwise.”
He noted that it has also strengthened Coos County Family Health Services’ relationships with community partners like Northern Human Services (mental health), the Family Resource Center, food/diaper banks and other community resource so they we are more aware of the services they can provide and therefore more likely to make referrals.
“Being more aware of trauma in general and its many negative impacts on the so-called social determinants of healthy also guides our day-to-day practice when issues arise because that possibility is already front and center in our thought process,” Dr. Beals said.
“Instead of making it into a negative experience we instead try to frame it more positively by turning the lens to reflect strengths and resiliency instead of focusing on challenges,” he concluded.
The work continues
The New Hampshire Children’s Health Foundation has funded additional work by the UNH Institute for Health Policy and Practice to conduct a second cohort to further expand trauma informed pediatric care. As of June, 2022, 17 additional introductory training sessions have been held or are scheduled and recruitment for a second cohort of Phase 2 practices has begun.
The New Hampshire Pediatric Improvement Partnership has published two resources to support pediatric primary care practices in building family resilience and addressing adverse childhood experiences.
Facilitating a Quality Improvement Approach to Childhood Adversity Screening in Primary Care: A Handbook provides a guide to replicating work done in the five New Hampshire practices to screen and respond to ACEs and strengthen family relationships.
A Guide to Trauma-informed Pediatric Primary Care provides a step-by-step process for clinics to develop and pilot a customized ACEs screening workflow, integrating principles of trauma-informed care.
The New Hampshire Pediatric Improvement Partnership is a collaborative effort of the Children’s Hospital at Dartmouth and the University of New Hampshire’s Institute for Health Policy and Practice.